
The oral collagen market is growing. So are the promises. And science, meanwhile, is becoming more stringent. A literature review published in early 2026 by Anglia Ruskin University covers 16 systematic reviews, 113 randomised controlled trials, and nearly 8,000 participants. Verdict: real benefits for skin and joints, no effect on sports performance, and serious methodological controversy that any B2B player should be aware of before crafting their narrative.
The largest synthesis to date — and what it really says about oral collagen
The ARU’s umbrella review is, to date, the most exhaustive synthesis available on oral collagen. It covers the skin, the musculoskeletal system, and sports performance in a single document.
The positive conclusions: supplementation is associated with statistically significant improvements in skin elasticity and hydration, and relief from osteoarthritis symptoms. The benefits appear with prolonged intake, as part of structural support – not a rapid surface cosmetic action.
What the study did not find: any significant reduction in skin roughness, improvement in athletic performance, or measurable gains in post-exercise recovery.
The authors are explicit: collagen can be positioned as a complementary tool for dermal support – particularly in menopausal women or in cases of photoageing – and not as a «face-lift in a capsule».
The grain of sand: an independent meta-analysis that changes the reading
This is where it gets complicated, and where B2B players need to be informed.
A meta-analysis published in 2025 in the’British Journal of Medicine applied a filter that few studies use: only retain trials of high methodological quality and Without industrial funding. Result — no significant effect on hydration, elasticity or wrinkles.
The message isn't that collagen doesn't work. It is the case that the magnitude of effects reported in the literature depends heavily on who is funding the studies. Industry-sponsored trials show positive effects. Independent and rigorous trials tend towards an absence of measurable clinical effect on skin ageing.
Osteoarthritis and musculoskeletal health: the strongest signal for oral collagen
On this ground, the literature is more coherent. The ARU umbrella review highlights a robust signal for osteoarthritis: clinically relevant improvements in pain and function scores. A dedicated meta-analysis from 2025 confirms that oral administration of collagen improves functional and pain scores in a statistically and clinically significant manner.
The data on muscle mass and tendon structure suggest modest — but heterogeneous — benefits that require confirmation by higher-powered studies.
A randomised trial from 2025 on knee osteoarthritis offers a counterpoint: the combination of undenatured type II collagen + hydrolysed collagen showed no significant difference compared to placebo in pain, function (KOOS score) or analgesic use over 12 weeks. These discrepancies between studies are likely explained by differences in formulation, dosage, intervention duration, patient phenotype, and design.
What this means for ingredient suppliers and brands
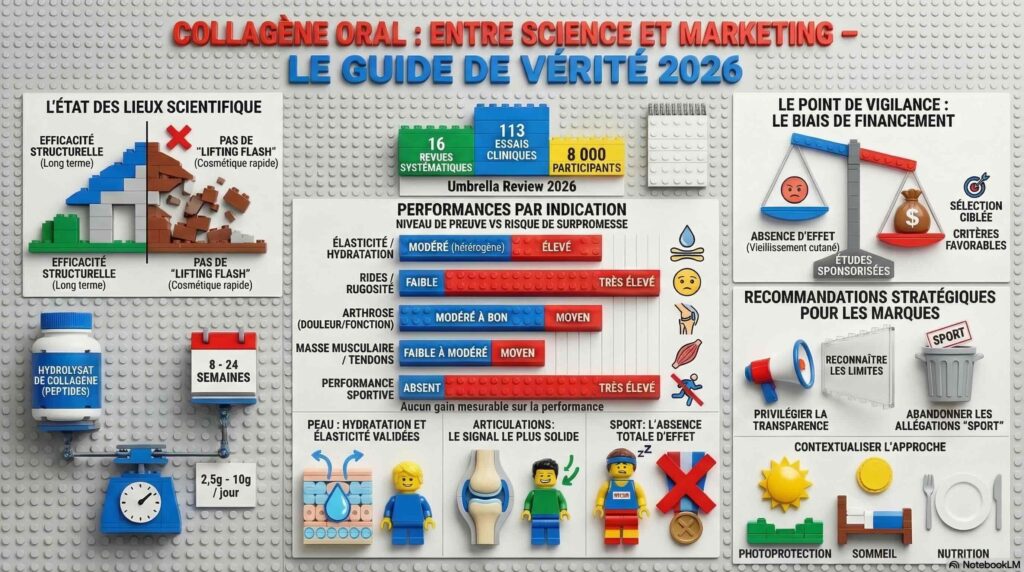
| Indication | Current level of evidence | Risk of over-promising |
| Skin elasticity / hydration | Moderate (heterogeneous, funding bias) | Raised |
| Rides / roughness | Weak (no effect in independent studies) | Very high |
| Arthrosis (pain, function) | Moderate to good | Medium |
| Muscle mass / tendons | Slight to moderate | Medium |
| Sports performance / recovery | Absent | Very high |
Sources: ARU umbrella review 2026 (DOI: 10.1093/asjof/ojag018); Am J Medicine 2025 (ScienceDirect); Nature Sci Rep 2025
Some concrete implications for the construction of the discourse produced:
Highlight the evidenced benefits with temporal considerations. Elasticity, hydration, joint relief — specifying that the effects are part of a long-term support strategy, not a rapid action.
Report the controversy rather than ignoring it. A speech that acknowledges the limitations of literature – and explains why your own data are methodologically sound – is more credible than one that glosses over the grey areas. Especially when dealing with an R&D buyer.
Abandon sports performance and recovery claims. The umbrella review is explicit. To continue using them is to expose oneself to immediate factual refutation.
Contextualise the collagen within a holistic approach. The president of the British Association of Dermatologists notes that most trials do not control for major factors of skin ageing – UV, smoking, sleep, hormonal status. Integrating collagen into a broader value proposition (photoprotection, nutrition, lifestyle) is both more honest and more differentiating.
Document your product features precisely. Type of collagen, degree of hydrolysis, dose, duration, target population. The divergences between studies are largely explained by these variables. A supplier capable of finely describing their ingredient and pointing to proprietary clinical data is positioned differently from those who aggregate the entire literature without distinction.
The real opportunity: rebuilding discourse on solid foundations
The oral collagen market is not going to slow down. Consumers and brands will continue to invest in it. What will change is the pressure for justification — regulatory, journalistic, and commercial.
B2B players who will get ahead in this transition are those who move from a generic «anti-ageing» promise to a proposition focused on documented structural support, with their own clinical data, precise population targeting, and discourse that integrates the nuances of the literature rather than evading them.
This is not a step backwards. It is a repositioning for greater credibility – which, in a market saturated with promises, becomes a genuine competitive advantage.
FAQ — What the pros really ask about oral collagen
Are all forms of collagen equivalent? No, and this is a key point of the controversy. Studies mix collagen hydrolysate (low molecular weight peptides), undenatured type II collagen, and other formulations, with varying doses and durations. The observed effects are not transferable from one form to another without specific data. A supplier who aggregates all the literature without differentiating between the forms takes a risk of overstating the effect.
What dose and for how long for a skin effect? Positive studies generally report effects from 2.5 to 10 g/day of collagen hydrolysate, over periods of 8 to 24 weeks. Below 8 weeks, the data is inconclusive. Duration is a key parameter that product communications often minimise.
Does food-grade collagen (bone broth, etc.) have the same effects? The available clinical data pertains to standardised supplemented forms, not to whole food sources. The bioavailability of active peptides from a non-standardised broth is difficult to estimate. This is an open question, not an acquired equivalence.
Why do sponsored trials give better results? This is a documented bias in the broader nutritional literature, not specific to collagen. It combines several mechanisms: selection of responsive populations, choice of favourable assessment criteria, durations adapted to the expected effect size, and selective publication of positive results. It is not necessarily fraud – it is methodological optimisation in service of a result.
Does EFSA's health claims regulation cover collagen? To date, no health claims under Regulation (EC) No 1924/2006 have been authorised for collagen or collagen peptides in Europe. Communications must therefore remain within the scope of generally accepted claims or be supported by studies for off-label indications. A subject to watch closely.
Video summary
Sources
- ARU Umbrella Review (2026). Aesthetic Surgery Journal Open Forum — https://academic.oup.com/asjopenforum/advance-article/doi/10.1093/asjof/ojag018/8446510
- Independent Meta-analysis (2025). British Journal of Medicine — https://www.sciencedirect.com/science/article/abs/pii/S0002934325002839
- Randomised trial osteoarthritis (2025). Nature Scientific Reports — https://www.nature.com/articles/s41598-025-17505-0
- PubMed — Collagen hydrolysate & skin (previous meta-analysis) — https://pubmed.ncbi.nlm.nih.gov/39212129/
- PubMed — Collagen & Joints (Meta-Analysis 2025) — https://pubmed.ncbi.nlm.nih.gov/40324552/
- Medical Xpress (02/2026) — https://medicalxpress.com/news/2026-02-collagen-benefits-skin.html
Are you promoting a collagen ingredient or building a narrative around healthy ageing?
→ Do you have a specific question? Our AI assistant can give you quick guidance: Talking to the assistant
→ Need structured support? Find out more about our formats - from one-shots to editorial partnerships: See the offers
→ Would you like to discuss it in person? 30 minutes to define your needs, with no obligation: Reserve a slot