Since their global commercial breakthrough, GLP-1 receptor agonists – semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro) – have proven to be game-changers far beyond the medical sphere. These molecules, initially prescribed for the treatment of type 2 diabetes and subsequently obesity, are profoundly altering users’ relationship with food: reduced appetite, altered taste preferences, intolerance to fatty or very sweet foods, and increased sensitivity to textures.
For nutrition professionals and stakeholders in the agri-food industry, this mass phenomenon represents a strategic signal of the highest importance. Understanding what users eat — and what they are looking for — GLP-1 has become a necessity for anticipating market needs, guiding reformulation strategies, and seizing new commercial opportunities.
Who are the users of GLP-1s today?
In 2026, the number of people on GLP-1 treatment worldwide is estimated to be in the tens of millions, primarily in North America, the UK and Western Europe. In Belgium and France, prescriptions are showing significant growth, despite supply shortages that marked the years 2023-2025.
The typical user profile is an adult aged 35 to 65, suffering from obesity or type 2 diabetes, often engaged in a comprehensive care pathway that includes nutritional monitoring, physical activity, and medical support. These consumers are generally well-informed, attentive to product composition, and open to functional foods, provided they meet their specific constraints: digestive tolerance, high nutritional density, and a format suited to a reduced appetite.
So it's not a passive consumer: it's a changing consumer, actively seeking products aligned with their treatment.
What food data reveals
Observational studies and data from food tracking apps converge towards a fairly consistent nutritional profile in GLP-1 users. Several clear trends are emerging.
Increased demand for high nutritional density
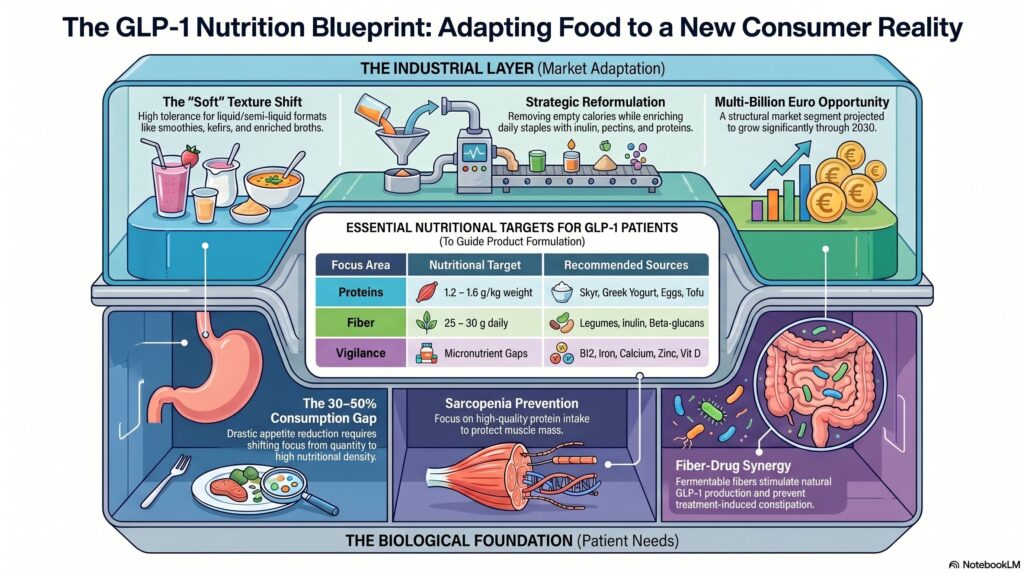
With a drastic reduction in the quantities consumed — often by 30 to 50 % compared with previous intake levels — every mouthful must «count». Users instinctively adopt a ‘quality over quantity’ approach: they prioritise foods rich in protein, fibre, vitamins and minerals, rather than empty calories.
2. A clear preference for light and digestible textures
Dense, very fatty, or very sugary foods are frequently poorly tolerated with GLP-1 treatment: nausea, reflux, and gastric discomfort are documented side effects. Users are massively turning to gentler options: plain yoghurts, kefir, vegetable soups, enriched broths, protein smoothies, fresh fruits, cooked vegetables, and lean fish. This trend towards «soft» textures and liquid or semi-liquid formats can be directly exploited by the agri-food industry.
3. Proteins, a nutritional imperative
Sarcopenia – the loss of muscle mass linked to caloric restriction – is one of the main nutritional risks associated with GLP-1 treatments. To counteract this, clinical recommendations emphasise sufficient protein intake, around 1.2 to 1.6g of protein per kg of body weight per day according to studies. In practice, this translates to increased consumption of dairy products (quark, Greek yoghurt, skyr), eggs, legumes, tofu, protein drinks, and protein-enriched snacks.
4. Fibre: An unexpected ally in treatment
One of the most promising results from recent research concerns the role of dietary fibre in the effectiveness of GLP-1 treatments. A review published in the journal Advances in Nutrition suggests that dietary fibre supplementation could be a complementary strategy to amplify the long-term effects of GLP-1 therapies on weight management. However, it should be noted that the weight loss achieved by fibre alone remains more modest than that induced by drug treatment: its role is primarily complementary, not substitutive. The mechanism is multifaceted: fermentable fibres nourish gut bacteria that produce short-chain fatty acids (SCFAs), which in turn stimulate the endogenous secretion of GLP-1 and other satiety hormones. In other words, eating more fibre could enhance and prolong the effects of drug treatment. Furthermore, fibre prevents constipation, a common side effect of GLP-1s often underestimated in general literature.
Tangible opportunities for the agri-food industry
This transformation in eating habits has not gone unnoticed by major manufacturers. Nestlé, Danone, Abbott Nutrition, and several sports nutrition brands have already begun repositioning existing ranges or developing new products specifically aimed at GLP-1 users.
- Reformulation of existing products Increasing the soluble fibre content (inulin, beta-glucans, pectins) and protein in everyday products – yoghurts, cereals, bars, soups – directly meets the expectations of this segment. The simultaneous reduction of added sugars and saturated fats reinforces the nutritional consistency of the positioning.
- Development of new formats GLP-1 users eat less, but more often. Nutritionally dense snacking – small, high-protein and fibrous packs, liquid or semi-liquid formats, enriched «mini-meals» – is a particularly promising area for innovation. Enriched collagen broths, kefir-based protein smoothies, and pre-portioned fibre shots illustrate this trend.
- Communication and claims Claims such as «high in fibre and protein,» «contributes to satiety,» and «suitable for a reduced diet» can resonate strongly with this segment, provided that the European regulatory framework for nutrition and health claims (Regulation EC 1924/2006) is strictly adhered to. Claims validated by the EFSA provide the most robust foundation for credible product communication.
What healthcare professionals need to remember
For dietitians-nutritionists, doctors, and pharmacists who are monitoring patients on GLP-1s, several points of vigilance are essential:
- Monitoring micronutrient deficiencies: Reduced food intake increases the risk of vitamin B12, iron, calcium, zinc, and vitamin D deficiency. Regular blood tests are recommended.
- Prioritise nutritional quality over simple calorie counting. Each meal should be designed to maximise the intake of essential nutrients.
- Alongside resistance physical activity (weight training, Pilates, Nordic walking) to preserve muscle mass during the weight loss phase.
- Integrate fibre as a complementary tool: 25 to 30g per day minimum, primarily targeting fermentable fibres with a prebiotic effect.
- Adapting dietary advice to individual tolerances: each patient reacts differently to treatment, and textures or foods that trigger nausea vary from person to person.
Conclusion
GLP-1 medications are not a passing trend: they are permanently reshaping millions of consumers' relationship with their diet. For the agri-food industry, this presents a major opportunity to create value by offering suitable products – richer in fibre and protein, easier to digest, and nutritionally impeccable. For healthcare professionals, it's a novel area of nutritional support, at the crossroads of pharmacology and dietetics. In both cases, those who prepare for it today will have a decisive head start.
FAQ — GLP-1 and Diet
Q1 — What is a GLP-1 medication and how does it affect eating habits?
GLP-1 (glucagon-like peptide-1) receptor agonists such as semaglutide (Ozempic, Wegovy) or tirzepatide (Mounjaro) are medications that mimic the behaviour of a natural gut hormone — GLP-1 — secreted after meals. They act on several mechanisms simultaneously: they slow down gastric emptying (which prolongs the feeling of fullness), reduce glucagon production, stimulate insulin secretion, and act on hunger centres in the brain. The result: a significant reduction in appetite, a change in food preferences, and, in most cases, gradual weight loss.
Q2 - What are the most recommended foods for GLP-1 users?
Foods with a high nutritional density and light texture are best suited. The following are particularly recommended: natural yoghurts and protein-rich dairy products (skyr, Greek yoghurt), eggs, legumes (lentils, chickpeas, beans), lean and fatty fish (salmon, mackerel), steamed vegetables, fresh, low-sugar fruits, fortified broths, and vegetable soups. These foods help to meet protein, fibre, and micronutrient requirements despite a significantly reduced food volume.
Q3 - Why are fibres particularly important during GLP-1 treatment?
Fibre plays a dual role in patients taking GLP-1s. On the one hand, it helps to prevent constipation, a common side effect of these medications. On the other hand, recent research suggests that fermentable fibres (prebiotics) could amplify the effects of the treatment by stimulating the endogenous production of GLP-1 by intestinal cells. This synergy between a fibre-rich diet and drug treatment is one of the most promising areas of research in current clinical nutrition.
Q4 — Are there any foods to absolutely avoid while on GLP-1 treatment?
Yes. Highly fatty foods (fried items, rich sauces, fatty cured meats), highly sugary foods (pastries, sugary drinks, sweets) and very spicy foods should be avoided as they often worsen nausea and digestive discomfort. Alcoholic drinks are also not recommended, as alcohol potentiates certain side effects and interferes with blood sugar regulation. In general, ultra-processed foods with low nutritional density should be limited as much as possible.
Q5 - What nutritional risks should be monitored in a patient on GLP-1s?
The main risk is protein-energy malnutrition and sarcopenia (muscle mass loss during weight loss). Deficiencies in vitamin B12, iron, calcium, zinc, and vitamin D have also been documented in long-term follow-up studies. Regular blood tests (at least every 6 months) are recommended for patients on prolonged treatment.
Q6 — Do «GLP-1 friendly» products represent a sustainable opportunity for the food industry?
Yes, without a doubt. With several tens of millions of active users worldwide and continuously growing prescriptions, this is not a fleeting niche but a structural market segment. Manufacturers who develop suitable products now – high nutritional density, rich in fibre and protein, light textures, small formats – are positioning themselves in a market estimated at several billion euros by 2030. The first reformulations observed at Nestlé, Danone, and several sports nutrition brands confirm that the momentum is already underway.
Reference
Dietary Fibre and GLP-1 Receptor Agonists in Obesity — ScienceDirect / Advances in Nutrition, 2026