
ADM values the female health market at $75.42 billion by 2033. Its white paper Elevating Women’s Health: Solutions for Every Step Compile market data, clinical references and formulation leads, from puberty to post-menopause. The document is robust and useful. It remains to be seen separately what falls under sector analysis and what falls under product argumentation.
public health women has become a strategic axis for functional ingredient suppliers. Sponsored white papers are multiplying, all presenting themselves as scientific, educational, and commercial resources. This triple role necessitates a methodical reading: what angle, what data selection, what purpose. ADM's document is a good example: serious, well-documented, driven by real scientific teams. It is precisely its quality that makes the sorting work all the more useful.
A market that no one wants to miss
The white paper opens with a market dynamic that few players would wish to miss. According to ADM, citing Grand View Research, the global women's health market would reach $75.42 billion by 2033 (CAGR of 5.1 per cent from Q3 to Q4 between 2026 and 2033), whilst the only market of the Menopause, estimated at 17.79 billion in 2024, is set to rise to 24.35 billion by 2030. The report also states that 60 % of women say they use vitamins, minerals or supplements to support their wellbeing goals. These figures are taken from the ADM report and its market sources; they should be cross-checked against primary reports before being used.
ADM is framing the opportunity around three trends:
- stage-of-life customisation,
- Proactive and holistic approach to health,
- Rise of so-called evidence-based solutions.
The document insists on the link between nutrition and mental health, reporting that 52 % of women associate a healthy lifestyle with good mental and emotional health, compared with 41 % of men. This is a relevant angle. It broadens the scope of functional ingredients far beyond traditional nutritional markers, extending to mood, sleep and cognition.
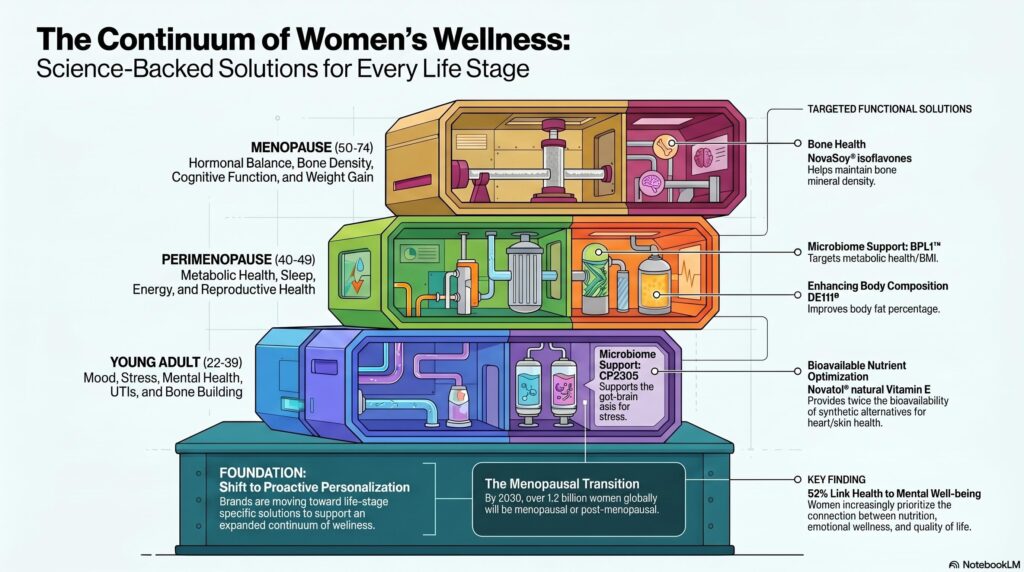
A coherent age segmentation, for commercial purposes as well
The document breaks down women's needs by age group. Stress, acne, urinary health, and bone development for ages 12-21. Fertility, energy, and metabolism for ages 22-39. Perimenopause, muscle mass, and sleep for ages 40-49. Menopause, hot flushes, cognition, and libido for ages 50-59. Then cardiovascular, bone, joint, and cognitive issues for those over 60.
Mapping reflects real physiological transitions. It also has a commercial function, which it acknowledges: linking each Need the state to a solution for the ADM portfolio. The document constructs a continuity between lifecycle and innovation pipeline, with an implicit promise: an ingredient solution for every key moment.
The point counts for a professional reader. This personalisation remains primarily structured by product categories and potential claims. Not yet clinical personalisation in the true sense. In practice, a woman's needs are not limited to an age or hormonal status. They depend on life context, nutritional status, comorbidities, psychosocial environment, and access to care. None of these determinants are formulated.
What the evidence really shows, ingredient by ingredient
This is where critical reading is won or lost. The white paper presents its ingredients in a single narrative dynamic, which can give an impression of homogeneous robustness. A separate reading reveals considerable maturity gaps.
| Ingredient | Indication highlighted by ADM | Key figure (as reported by ADM) | Maturity of the evidence |
| L. gasseri CP2305 (postbiotic) | Sleep, stress, mood, PMS, menopausal symptoms | Time to wakefulness after falling asleep: 23→18 mins vs 23→22 mins on placebo (−18.5 %), 24-week trial | A genuine indication on the stress-sleep axis. Data lacking in detail, limited timeframes, and predominantly subjective criteria |
| BPL1 — B. animalis lactis CECT8145 (pro/postbiotic) | Waist circumference, BMI, visceral fat | −1.75 cm (pro) / −1.9 cm (post) vs −0.19 cm placebo; 135 adults, 12 weeks | Beneficial but modest and short-term effects. Role of diet and activity not discussed |
| Esflorin1 B. longum CECT7347 (pro/postbiotic) | Irritable Bowel Syndrome with a predominant diarrhoeic component | IBS-SSS improved ~3× vs placebo; 200 adults, 12 weeks | More robust dossier, endpoints consistent with the indication. Study not presented as specifically feminine |
| Fibersol (soluble prebiotic fibre) | Digestion, satiety, GLP-1/PYY, blood glucose | Over 30 years of research, over 100 publications cited | Solid foundation for multiple uses. Specificity of «women's health» more narrative than demonstrated. |
| Novasoy — Soya isoflavones | Hot flushes, bone health, cognition | EFSA: doses of 35 to 100 mg/day deemed safe for peri/post-menopause; >10,000 publications | The most mature level of evidence in the file |
| Novatol — Natural Vitamin E | Cardiovascular, immunity, cognition, skin, eye | Bioavailability x2 compared with synthetic forms; 67 % of the population receiving the supplements (ADM claims) | Real nutritional foundation. Risk of marketing extension towards beauty and anti-ageing. |
Two readings are essential. The first: CP2305 and BPL1 are based on interesting but fragile signals, where statistical significance is emphasised far more than effect size, clinical relevance, or independent reproducibility. The second: isoflavones and vitamin E benefit from a broad historical basis, but this basis does not specifically bear the ADM mark, nor does it allow the argument to be extended to unproven cosmetic benefits.
A telling detail runs through the entire file. Several studies cited are not conducted on specifically female populations. They are recontextualised within a «women's health» narrative. The question to ask systematically: is the evidence specifically female, or recontextualised within a «women's health» narrative?
Three points of vigilance to keep in mind when reading
The first sticks to its ingredient-centric logic. Women’s health becomes a succession of symptoms to be addressed by a formulated solution. The overall quality of diet, physical activity, mental load, socio-economic status, and access to diagnosis: these major determinants are almost absent from the narrative.
The second It is methodological. The document juxtaposes a pilot trial, an exploratory study, a robust randomised trial, a review and market data without explicit prioritisation of the level of evidence. The coexistence creates an impression of convergence superior to reality.
The third It's communicative. Phrases like «backed by science», «clinically documented», and «evidence-based solutions» are valuable. However, they never absolve you from examining the publications, populations, endpoints, and effect size. In a field as heterogeneous as women's health, this simplification can lead to shortcuts that careful reading avoids.
What the document implies about the market
Beyond its limitations, the white paper documents a real transformation. Women's health is no longer addressed solely through the lens of deficiencies or reproduction, but as a continuum encompassing metabolism, digestion, mood, sleep, cognition, sexuality, skin, the microbiome, and ageing. The expansion of the scope creates opportunities for innovation. It also increases the risk of scientific dilution.
Le microbiome y becomes a quasi-universal explanatory framework. Stress, sleep, menopause, weight, vaginal health, digestion: the gut-brain axis and microbial ecology serve as a unifying narrative framework, capable of connecting disparate offerings under a single innovation story. Unifying from the supply side. Demanding from the evidence side. The more universal a framework becomes, the greater the risk of extrapolation.
For a specialist media outlet, a brand or a consultant, this type of document retains significant practical value. It captures the industrial narratives in circulation, the suppliers' formulation arguments, and the ingredients on which differentiation is focused. The reflex to maintain: go back to the primary sources, separate contextual data from portfolio-oriented messages, examine each ingredient on its own merits, and verify regulatory compliance — which ADM itself reminds you of, specifying that no claims are approved by the authorities and that responsibility lies with the manufacturer of the finished product.
In B2B communication, as in popularisation, value lies not in the multiplication of promises. It lies in the ability to qualify levels of proof, areas of uncertainty, and concrete usage conditions. What is the next study you would demand before transforming one of these signals into an allegation?
FAQ
Is this white paper useful despite being sponsored?
Yes. It brings together market data, consumer trends, clinical references, and a structured overview of ingredients promoted for women's health into one document. Its benefit: mapping the sector's priorities, provided it's kept in mind that it's also designed to showcase ADM's solutions.
Do all the presented ingredients have the same level of evidence?
No. The spectrum ranges from small exploratory trials (certain recent strains) to mature dossiers (soy isoflavones, certain fibres). The uniform presentation smoothes over these disparities; reading ingredient by ingredient reveals them.
Can the benefits highlighted in brand communication be directly adopted?
No, not without thorough verification. The document itself recalls that the ingredients may not be available everywhere, that claims depend on local regulations, and that no statement is made as approved by the authorities.
What is the key takeaway message for nutrition professionals?
Women's health has become a strategic territory, with a strong focus on the microbiome, mood, sleep, menopause, and metabolic health. However, credible communication distinguishes clinical signal, practical relevance, usage context, and actual level of evidence – rather than converting every positive study into a generalised promise.
References cited by ADM
The figures and studies mentioned originate from the ADM white paper and its own references. They must be verified with the primary sources before any reuse.
- [1] Admiral. Elevating Women’s Health: Solutions for Every Step (Sponsored white paper).
- [2] Grand View Research – Women's Health and Menopause Market Data (cited by ADM).
- [3] Mintel, Innova, Euromonitor — consumer trends (cited by ADM).
- [4] Nishida et al. ; Sawada et al. — Lactobacillus gasseri CP2305 (cited by ADM).
- [5] Pedret et al. — BPL1 / B. animalis lactis CECT8145 (cited by ADM).
- [6] Srivastava et al. — Esflorin1 / B. longum CECT7347 (cited by ADM).
- [7] Ye et al. ; Yuasa et al. — Fibersol (cited by ADM).
- [8] Messina et al.; EFSA — soy isoflavones, safe dose 35-100 mg/day peri/post-menopause (cited by ADM).
- [9] Passarelli et al. — insufficient vitamin E intake (cited by ADM).
- Public health sources mentioned: UNICEF, The Menopause Society, Endocrine Society, Mayo Clinic, Office of Dietary Supplements.